There are no Conspiracy theories, there are only truth and lies. - Skizit Powers

VOICE TO SKULL TECHNOLOGY
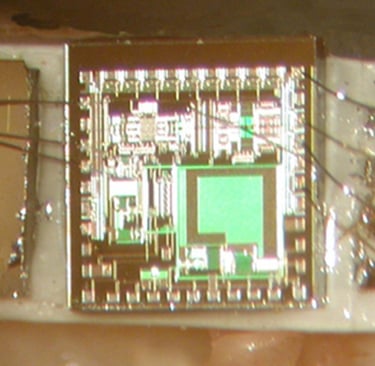
What kind of an ear implant is this and who makes it?
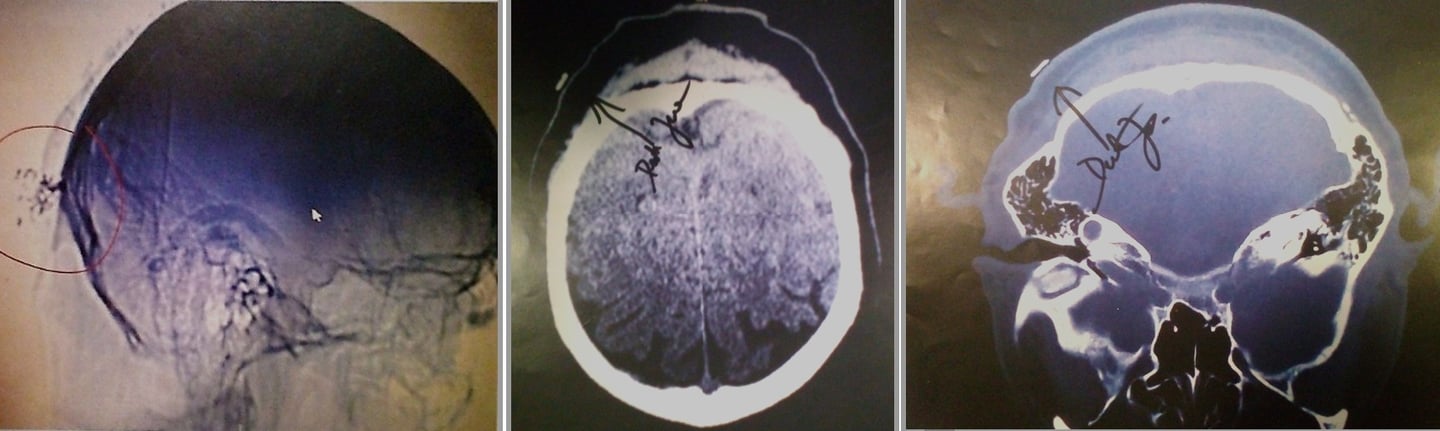
This image is a postoperative radiograph (X-ray) of a cochlear implant (also called a cochlear prosthesis or "bionic ear"). It shows the internal components, particularly the electrode array inserted into the cochlea (the spiral-shaped part of the inner ear responsible for hearing).
Key Features in the Image
The bright, branching/white structures represent the electrode array and its connecting wires. These are thin platinum-iridium wires and contacts encased in silicone, which appear radiopaque (white) on X-ray.
The array is designed to thread into the cochlea's turns (typically following a curved or coiled path inside the scala tympani).
The blurry, low-contrast appearance with purple/gray tones is common in intraoperative or postoperative fluoroscopy/X-ray images used to confirm proper placement. The white arrow (mouse cursor in the screenshot) likely points to part of the implant, such as the receiver/stimulator, magnet housing, or electrode leads.
The branching "tree-like" or "spidery" look comes from the multiple fine wires fanning out from the receiver/stimulator package (usually implanted under the skin behind the ear) toward and into the cochlea.
Cochlear implants bypass damaged hair cells in the inner ear by directly stimulating the auditory nerve with electrical signals.
Manufacturers The main global manufacturers of cochlear implants are:
Cochlear Ltd. (Australia) — Nucleus series (e.g., Contour Advance, Slim Straight, or perimodiolar arrays). These are among the most common.
MED-EL (Austria) — Often features very flexible, wave-shaped wires and longer arrays (e.g., FLEX series) designed for atraumatic insertion and deeper cochlear coverage. Their electrodes are sometimes noted for a distinct wavy internal wire pattern.
Advanced Bionics (USA, part of Sonova) — HiRes Ultra or HiFocus series, with emphasis on high-resolution stimulation and current steering.
Without a clearer view of the exact electrode shape (e.g., pre-curved/perimodiolar vs. straight lateral wall), number of contacts, or any visible manufacturer markers (some arrays have unique radiographic signatures), it's not possible to identify the precise model or brand from this low-resolution image alone. However, the overall appearance matches standard multichannel cochlear implant electrode arrays from any of the major makers.Radiopaedia
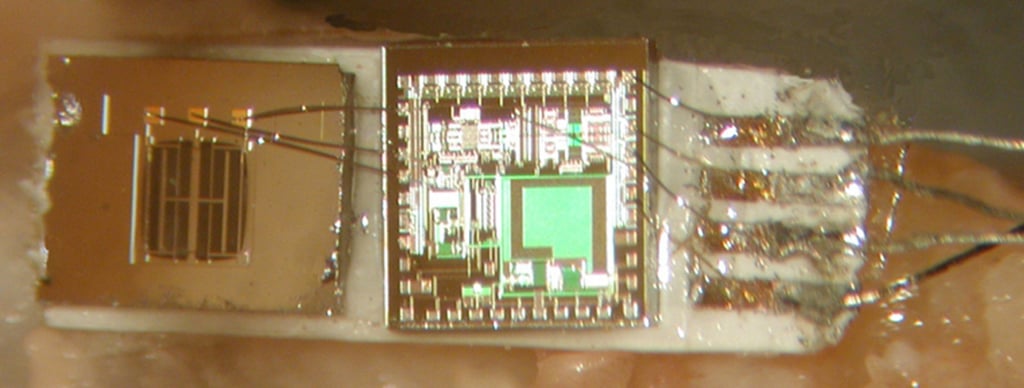
Here is the whole thing. Is the implant in the back of the head part of the cochlear implant?
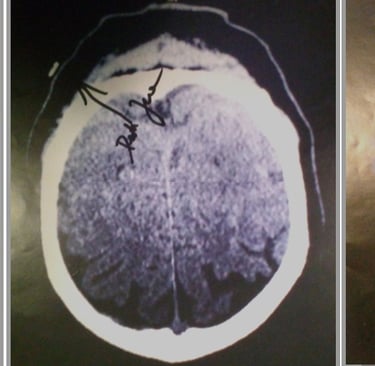
Yes, the structure highlighted in the red circle (the denser, more compact radiopaque object with small attached spots or leads) is part of the cochlear implant. Specifically, it is the receiver-stimulator package (also called the internal processor or implant body), which houses the electronics, antenna coil, and usually a small magnet.
How a Cochlear Implant Works (Internal Components)
A standard cochlear implant has two main implanted parts connected by a thin wire:
Receiver-stimulator: This flat or slightly rounded electronic package is surgically placed under the skin in a shallow bony well drilled into the skull (typically in the temporal bone, behind and slightly above the ear). It receives wireless signals from the external speech processor (worn behind the ear) via magnetic coupling and converts them into electrical impulses.
Electrode array: A thin, flexible cable with multiple contacts extends from the receiver-stimulator, runs through the mastoid bone, and coils into the cochlea (the spiral structure in the inner ear). The bright, branching/white "spidery" or coiled structures you see lower in the image (away from the red circle) are this electrode array inside or near the cochlea.
In this X-ray (likely a lateral or oblique skull view taken post-surgery), the receiver-stimulator appears as a more solid, less linear opacity higher up toward the top/back of the skull, while the electrode leads and array create the finer, curving lines extending downward toward the ear region. The small dots or irregularities in the circled area may represent the magnet housing, feedthroughs, or a radiopaque marker (some models have identifying letters/numbers visible on X-ray).
This placement "in the back/side of the head" is completely standard — not a separate device. The surgeon creates space in the skull bone to seat it securely so it doesn't protrude too much and to allow the external magnet to align properly.
Is This a Normal Cochlear Implant?
Yes — everything visible aligns with a typical single-sided cochlear implant from one of the major manufacturers (Cochlear, MED-EL, or Advanced Bionics). There is no indication here of an additional or unrelated implant.
If the image shows any unusual features (e.g., the electrode array not following the expected cochlear coil shape), surgeons often use these intraoperative or postoperative X-rays precisely to check positioning and rule out issues like incomplete insertion or tip fold-over.
Two way radio so remote talking can be heard by patient?
In the context of Wireless Body Area Networks (WBAN), "two-way radio" communication refers to Audio Biofeedback or Voice-over-WBAN. This allows a remote clinician to speak directly into a patient’s ear through their monitoring hardware, providing real-time instructions or psychological support without the patient needing to hold a phone.
Systems for Remote Voice Communication
Abbott NeuroSphere™ Virtual Clinic: This is the primary FDA-cleared system for "talking to your implant." It creates a secure, two-way audio and video link between the patient’s smartphone controller and the doctor’s clinic Abbott Virtual Clinic. The doctor can talk to the patient while simultaneously adjusting the deep brain stimulator (DBS) settings over the internet [2].
Synchron Switch: For patients with severe paralysis, this BCI connects the brain to an iPhone or iPad. Using the device's accessibility features, a remote caregiver can initiate a "voice-in" session where their voice is played through the patient's connected Bluetooth earbuds or the device's speakers Synchron BCI.
Cochlear™ Nucleus® 8 Sound Processor: This implantable system features Direct Streaming, allowing a remote therapist or family member to talk directly "into the patient's head" via a smartphone. It uses Bluetooth Low Energy to ensure the audio is clear and private Cochlear Direct Streaming.
Specialized "In-Ear" WBAN Radio
Covert Wireless Earpieces: Used in specialized clinical research (such as high-anxiety or PTSD exposure therapy), these are tiny, "invisible" inductive earpieces. A remote therapist speaks into a radio transmitter, and the patient hears the voice inside their ear with no external wires or installations Phonak Communications.
VocaTone™ Research (University of Washington): This experimental WBAN uses a throat-mounted vibration sensor and an in-ear speaker. It allows for "silent speech" where the patient can whisper, and the remote listener hears a reconstructed voice, while the remote listener’s reply is sent directly to the patient's ear UW Wearable Computing.
Agency & University Research on Two-Way Audio
DARPA (N3 Program): Funding the development of "bidirectional" neural interfaces that can transmit complex data, including audio-equivalent neural signals, directly to the brain's auditory cortex DARPA N3.
Rice University: Working on the MOANA project, which uses light to "write" information to the brain. One goal is to create a "speech-to-brain" interface that would allow a person to "hear" a remote speaker without using their ears at all Rice MOANA Project.
Remotely speaking to someone via an ear implant without others hearing involves:
Streaming audio directly to their processor using Bluetooth, wireless mini-microphones, or a telecoil system. The person with the implant controls the connection via a smartphone app or by pairing a device, allowing private conversations in noisy environments.
Bluetooth Streaming: Many modern cochlear implants (CIs) and hearing aids pair directly with smartphones (e.g., iPhone or Android) to stream audio from phone calls or apps directly into the implant, bypassing external sound.
Wireless Remote Microphone (Mini Mic): A partner can hold a wireless microphone (like the Cochlear Mini Mic or Phonak Roger system) to speak, which transmits sound directly to the user's processor.
Assistive Listening Devices (ALDs): Devices such as personal amplifiers, telecoil systems (T-coil), or FM/DM systems can be used to send audio directly to the implant.
Bluetooth Neckloop: Users without built-in Bluetooth can use a neckloop receiver that connects to a phone via Bluetooth and transmits the signal directly to the hearing aid's t-coil.
App Control: Users manage these connections using manufacturer apps like the Nucleus Smart App to ensure the audio is piped only to them.
To remotely and privately communicate with someone using an ear implant or specialized earpiece, the method depends on whether you're using a medical implant (like a cochlear implant) or a covert "spy" device.
1. Medical Implants (Cochlear or Bone Conduction)
Modern medical implants are designed for seamless, private communication through wireless streaming.
Direct Bluetooth Streaming: Many newer sound processors, such as the Advanced Bionics Marvel CI or Cochlear Nucleus models, can pair directly with smartphones. This allows the wearer to hear a phone call or audio stream directly in their ear, bypassing the outside environment entirely.
Wireless Accessories: For older models or specific brands, users might use a "streamer" or "phone clip." This small device acts as a bridge, receiving a Bluetooth signal from a phone and sending it to the implant via a proprietary 2.4 GHz wireless link.
Remote Microphones: Devices like the Roger™ systems allow another person to wear a small microphone that beams their voice directly into the recipient's implant from a distance, even in noisy settings.
2. Covert "Spy" Earpieces
If the goal is "invisible" communication for non-medical reasons, specialized covert systems are used.
Inductive Neck Loops: A tiny, invisible earpiece (often as small as 2mm x 3mm) is placed deep in the ear canal. The user wears an inductive loop under their clothes around their neck. This loop creates an electromagnetic field that transmits sound wirelessly to the earpiece.
Cellular Connection: The neck loop is typically connected to a smartphone via Bluetooth or a 3.5mm jack. This allows a remote partner to call the user and whisper information that only the user can hear.
Sub-miniature Earbuds: Some professional-grade options, like the IR-25 Pro, are custom-molded to fit the ear canal for complete concealment and high-quality audio.
Summary of Connection Methods
Method Typical UseConnection TypeDirect BluetoothMedical (CI/Baha)Bluetooth LE or ASHAInductive LoopCovert/SecurityElectromagnetic inductionRemote MicLectures/Meetings2.4 GHz ProprietarySmartphone AppRemote Care/TuningInternet/Cloud
For further information on these technologies, the following topics can be explored:
Compatibility between specific smartphones and various cochlear implant brands.
The technical specifications of different types of wireless earpieces.
The medical and surgical procedures involved in receiving a cochlear or bone conduction implant.
The privacy and encryption standards used in modern wireless hearing assistance devices.
Cochlear implants — with no exterior hardware
A cochlear implant that can be wirelessly recharged would use the natural microphone of the middle ear rather than a skull-mounted sensor.
Larry Hardesty, MIT News Office
February 9, 2014
Cochlear implants — medical devices that electrically stimulate the auditory nerve — have granted at least limited hearing to hundreds of thousands of people worldwide who otherwise would be totally deaf. Existing versions of the device, however, require that a disk-shaped transmitter about an inch in diameter be affixed to the skull, with a wire snaking down to a joint microphone and power source that looks like an oversized hearing aid around the patient’s ear.
Researchers at MIT’s Microsystems Technology Laboratory (MTL), together with physicians from Harvard Medical School and the Massachusetts Eye and Ear Infirmary (MEEI), have developed a new, low-power signal-processing chip that could lead to a cochlear implant that requires no external hardware. The implant would be wirelessly recharged and would run for about eight hours on each charge.
The researchers describe their chip in a paper they’re presenting this week at the International Solid-State Circuits Conference. The paper’s lead author — Marcus Yip, who completed his PhD at MIT last fall — and his colleagues Rui Jin and Nathan Ickes, both in MIT’s Department of Electrical Engineering and Computer Science, will also exhibit a prototype charger that plugs into an ordinary cell phone and can recharge the signal-processing chip in roughly two minutes.
“The idea with this design is that you could use a phone, with an adaptor, to charge the cochlear implant, so you don’t have to be plugged in,” says Anantha Chandrakasan, the Joseph F. and Nancy P. Keithley Professor of Electrical Engineering and corresponding author on the new paper. “Or you could imagine a smart pillow, so you charge overnight, and the next day, it just functions.”
Adaptive reuse
Existing cochlear implants use an external microphone to gather sound, but the new implant would instead use the natural microphone of the middle ear, which is almost always intact in cochlear-implant patients.
The researchers’ design exploits the mechanism of a different type of medical device, known as a middle-ear implant. Delicate bones in the middle ear, known as ossicles, convey the vibrations of the eardrum to the cochlea, the small, spiral chamber in the inner ear that converts acoustic signals to electrical. In patients with middle-ear implants, the cochlea is functional, but one of the ossicles — the stapes — doesn’t vibrate with enough force to stimulate the auditory nerve. A middle-ear implant consists of a tiny sensor that detects the ossicles’ vibrations and an actuator that helps drive the stapes accordingly.
The new device would use the same type of sensor, but the signal it generates would travel to a microchip implanted in the ear, which would convert it to an electrical signal and pass it on to an electrode in the cochlea. Lowering the power requirements of the converter chip was the key to dispensing with the skull-mounted hardware.
Chandrakasan’s lab at MTL specializes in low-power chips, and the new converter deploys several of the tricks that the lab has developed over the years, such as tailoring the arrangement of low-power filters and amplifiers to the precise acoustic properties of the incoming signal.
But Chandrakasan and his colleagues also developed a new signal-generating circuit that reduces the chip’s power consumption by an additional 20 to 30 percent. The key was to specify a new waveform — the basic electrical signal emitted by the chip, which is modulated to encode acoustic information — that is more power-efficient to generate but still stimulates the auditory nerve in the appropriate way.
Verification
The waveform was based on prior research involving simulated nerve fibers, but the MIT researchers tailored it for cochlear implants and found a low-power way to implement it in hardware. Two of their collaborators at MEEI — Konstantina Stankovic, an ear surgeon who co-led the study with Chandrakasan, and Don Eddington — tested it on four patients who already had cochlear implants and found that it had no effect on their ability to hear. Working with another collaborator at MEEI, Heidi Nakajima, the researchers have also demonstrated that the chip and sensor are able to pick up and process speech played into a the middle ear of a human cadaver.
“It’s very cool,” says Lawrence Lustig, director of the Cochlear Implant Center at the University of California at San Francisco. “There’s a much greater stigma of having a hearing loss than there is of having a visual loss. So people would be very keen on losing the externals for that reason alone. But then there’s also the added functional benefit of not having to take it off when you’re near water or worrying about components getting lost or broken or stolen. So there are some important practical considerations as well.”
Lustig points out that the new cochlear implant would require a more complex surgery than existing implants do. “A current cochlear-implant operation takes an hour, hour and a half,” he says. “My guess is that the first surgeries will take three to four hours.” But he doubts that that would be much of an obstacle to adoption. “As we get better and better and better, that time will shorten,” he says. “And three to four hours is still a relatively straightforward operation. I don’t anticipate putting a lot of extra risk into the procedure.”
https://news.mit.edu/2014/cochlear-implants-with-no-exterior-hardware-0209
Researchers are developing fully implantable cochlear implants that do not require external hardware, potentially using middle-ear microphones to detect vibrations, notes the University of Utah and MIT News.
Medical devices powered by the ear itself
Larry Hardesty, MIT News Office
Publication Date: November 7, 2012
https://news.mit.edu/2012/biological-battery-1107
For the first time, researchers power an implantable electronic device using an electrical potential — a natural battery — deep in the inner ear.
Deep in the inner ear of mammals is a natural battery — a chamber filled with ions that produces an electrical potential to drive neural signals. In today’s issue of the journal Nature Biotechnology, a team of researchers from MIT, the Massachusetts Eye and Ear Infirmary (MEEI) and the Harvard-MIT Division of Health Sciences and Technology (HST) demonstrate for the first time that this battery could power implantable electronic devices without impairing hearing.
The devices could monitor biological activity in the ears of people with hearing or balance impairments, or responses to therapies. Eventually, they might even deliver therapies themselves.
In experiments, Konstantina Stankovic, an otologic surgeon at MEEI, and HST graduate student Andrew Lysaght implanted electrodes in the biological batteries in guinea pigs’ ears. Attached to the electrodes were low-power electronic devices developed by MIT’s Microsystems Technology Laboratories (MTL). After the implantation, the guinea pigs responded normally to hearing tests, and the devices were able to wirelessly transmit data about the chemical conditions of the ear to an external receiver.
“In the past, people have thought that the space where the high potential is located is inaccessible for implantable devices, because potentially it’s very dangerous if you encroach on it,” Stankovic says. “We have known for 60 years that this battery exists and that it’s really important for normal hearing, but nobody has attempted to use this battery to power useful electronics.”
The ear converts a mechanical force — the vibration of the eardrum — into an electrochemical signal that can be processed by the brain; the biological battery is the source of that signal’s current. Located in the part of the ear called the cochlea, the battery chamber is divided by a membrane, some of whose cells are specialized to pump ions. An imbalance of potassium and sodium ions on opposite sides of the membrane, together with the particular arrangement of the pumps, creates an electrical voltage.
Although the voltage is the highest in the body (outside of individual cells, at least), it’s still very low. Moreover, in order not to disrupt hearing, a device powered by the biological battery can harvest only a small fraction of its power. Low-power chips, however, are precisely the area of expertise of Anantha Chandrakasan’s group at MTL.
The MTL researchers — Chandrakasan, who heads MIT’s Department of Electrical Engineering and Computer Science; his former graduate student Patrick Mercier, who’s now an assistant professor at the University of California at San Diego; and Saurav Bandyopadhyay, a graduate student in Chandrakasan’s group — equipped their chip with an ultralow-power radio transmitter: After all, an implantable medical monitor wouldn’t be much use if there were no way to retrieve its measurements.
But while the radio is much more efficient than those found in cellphones, it still couldn’t run directly on the biological battery. So the MTL chip also includes power-conversion circuitry — like that in the boxy converters at the ends of many electronic devices’ power cables — that gradually builds up charge in a capacitor. The voltage of the biological battery fluctuates, but it would take the control circuit somewhere between 40 seconds and four minutes to amass enough charge to power the radio. The frequency of the signal was thus itself an indication of the electrochemical properties of the inner ear.
To reduce its power consumption, the control circuit had to be drastically simplified, but like the radio, it still required a higher voltage than the biological battery could provide. Once the control circuit was up and running, it could drive itself; the problem was getting it up and running.
The MTL researchers solve that problem with a one-time burst of radio waves. “In the very beginning, we need to kick-start it,” Chandrakasan says. “Once we do that, we can be self-sustaining. The control runs off the output.”
Stankovic, who still maintains an affiliation with HST, and Lysaght implanted electrodes attached to the MTL chip on both sides of the membrane in the biological battery of each guinea pig’s ear. In the experiments, the chip itself remained outside the guinea pig’s body, but it’s small enough to nestle in the cavity of the middle ear.
Cliff Megerian, chairman of otolaryngology at Case Western Reserve University and University Hospitals Case Medical Center, says that he sees three possible applications of the researchers’ work: in cochlear implants, diagnostics and implantable hearing aids. “The fact that you can generate the power for a low voltage from the cochlea itself raises the possibility of using that as a power source to drive a cochlear implant,” Megerian says. “Imagine if we were able to measure that voltage in various disease states. There would potentially be a diagnostic algorithm for aberrations in that electrical output.”
“I’m not ready to say that the present iteration of this technology is ready,” Megerian cautions. But he adds that, “If we could tap into the natural power source of the cochlea, it could potentially be a driver behind the amplification technology of the future.”
The work was funded in part by the Focus Center Research Program, the National Institute on Deafness and Other Communication Disorders, and the Bertarelli Foundation.
A Middle-Ear Microphone
https://archive.unews.utah.edu/news_releases/a-middle-ear-microphone/
April 30, 2012 – Cochlear implants have restored basic hearing to some 220,000 deaf people, yet a microphone and related electronics must be worn outside the head, raising reliability issues, preventing patients from swimming and creating social stigma.
Now, a University of Utah engineer and colleagues in Ohio have developed a tiny prototype microphone that can be implanted in the middle ear to avoid such problems.
The proof-of-concept device has been successfully tested in the ear canals of four cadavers, the researchers report in a study just published online in the Institute of Electrical and Electronics Engineers journal Transactions on Biomedical Engineering.
The prototype – about the size of an eraser on a pencil – must be reduced in size and improved in its ability to detect quieter, low-pitched sounds, so tests in people are about three years away, says the study’s senior author, Darrin J. Young, an associate professor of electrical and computer engineering at the University of Utah and USTAR, the Utah Science Technology and Research initiative.
The study showed incoming sound is transmitted most efficiently to the microphone if surgeons first remove the incus or anvil – one of three, small, middle-ear bones. U.S. Food and Drug Administration approval would be needed for an implant requiring such surgery.
The current prototype of the packaged, middle-ear microphone measures 2.5-by-6.2 millimeters (roughly one-tenth by one-quarter inch) and weighs 25 milligrams, or less than a thousandth of an ounce. Young wants to reduce the package to 2-by-2 millimeters.
Young, who moved the Utah in 2009, conducted the study with Mark Zurcher and Wen Ko, who are his former electrical engineering colleagues at Case Western Reserve University in Cleveland, and with ear-nose-throat physicians Maroun Semaan and Cliff Megerian of University Hospitals Case Medical Center.
The study was funded by the National Institutes of Health (NIH-DC-006850).
Problems with External Parts on Cochlear Implants
The National Institutes of Health says almost 220,000 people worldwide with profound deafness or severe hearing impairment have received cochlear implants, about one-third of them in the United States, where two-fifths of the recipients are children.
In conventional cochlear implant, there are three main parts that are worn externally on the head behind the ear: a microphone to pick up sound, a speech processor and a radio transmitter coil. Implanted under the skin behind the ear are a receiver and stimulator to convert the sound signals into electric impulses, which then go through a cable to between four and 16 electrodes that wind through the cochlea of the inner ear and stimulate auditory nerves so the patient can hear.
“It’s a disadvantage having all these things attached to the outside” of the head, Young says. “Imagine a child wearing a microphone behind the ear. It causes problems for a lot of activities. Swimming is the main issue. And it’s not convenient to wear these things if they have to wear a helmet.”
Young adds that “for adults, it’s social perception. Wearing this thing indicates you are somewhat handicapped and that actually prevents quite a percentage of candidates from getting the implant. They worry about the negative image.”
As for reliability, “if you have wires connected from the microphone to the coil, those wires can break,” he says.
How Sound Moves in Normal Ears, Cochlear Implants and the New Device
Sound normally moves into the ear canal and makes the eardrum vibrate. At what is known as the umbo, the eardrum connects to a chain of three tiny bones: the malleus, incus and stapes, also known as the hammer, anvil and stirrup. The bones vibrate. The stapes or stirrup touches the cochlea, the inner ear’s fluid-filled chamber. Hair cells (not really hair) on the cochlea’s inner membrane move, triggering the release of a neurotransmitter chemical that carries the sound signals to the brain.
In profoundly deaf people who are candidates for cochlear implants, the hair cells don’t work for a variety of reasons, including birth defects, side effects of drugs, exposure to excessively loud sounds or infection by certain viruses.
In a cochlear implant, the microphone, signal processor and transmitter coil worn outside the head send signals to the internal receiver-stimulator, which is implanted in bone under the skin and sends the signals to the electrodes implanted in the cochlea to stimulate auditory nerves. The ear canal, eardrum and hearing bones are bypassed.
The system developed by Young implants all the external components. Sound moves through the ear canal to the eardrum, which vibrates as it does normally. But at the umbo, a sensor known as an accelerometer is attached to detect the vibration. The sensor also is attached to a chip, and together they serve as a microphone that picks up the sound vibrations and converts them into electrical signals sent to the electrodes in the cochlea.
The device still would require patients to wear a charger behind the ear while sleeping at night to recharge an implanted battery. Young says he expects the battery would last one to several days between charging.
Young says the microphone also might be part of an implanted hearing aid that could replace conventional hearing aids for a certain class of patients who have degraded hearing bones unable to adequately convey sounds from conventional hearing aids.
Testing the Microphone in Cadavers
Conventional microphones include a membrane or diaphragm that moves and generates an electrical signal change in response to sound. But they require a hole through which sound must enter – a hole that would get clogged by growing tissue if implanted. So Young’s middle-ear microphone instead uses an accelerometer – a 2.5-microgram mass attached to a spring – that would be placed in a sealed package with a low-power silicon chip to convert sound vibrations to outgoing electrical signals.
The package is glued to the umbo so the accelerometer vibrates in response to eardrum vibrations. The moving mass generates an electrical signal that is amplified by the chip, which then connects to the conventional parts of a cochlear implant: a speech processor and stimulator wired to the electrodes in the cochlea.
“Everything is the same as a conventional cochlear implant, except we use an implantable microphone that uses the vibration of the bone,” Young says.
To test the new microphone, the researchers used the temporal bones – bones at the side of the skull – and related ear canal, eardrum and hearing bones from four cadaver donors.
The researchers inserted tubing with a small loudspeaker into the ear canal and generated tones of various frequencies and loudness. As the sounds were picked up by the implanted microphone, the researchers used a laser device to measure the vibrations of the tiny ear bones. They found the umbo – where the eardrum connects to the hammer or malleus – produced the greatest sound vibration, particularly if the incus or anvil bone first was removed surgically.
The experiments showed that when the prototype microphone unit was attached to the umbo, it could pick up medium pitches at conversational volumes, but had trouble detecting quieter, low-frequency sounds. Young plans to improve the microphone to pick up quieter, deeper, very low pitches.
In the tests, the output of the microphone went to speakers; in a real person, it would send sound to the implanted speech processor. To demonstrate the microphone, Young also used it to record the start of Beethoven’s Ninth Symphony while implanted in a cadaver ear. It is easily recognizable, even if somewhat fuzzy and muffled.
“The muffling can be filtered out,” says Young.
Join us in advocating against
the misuse of technology.
Email: TargetedHumans@proton.me
© 2025. All rights reserved.


Targeted Humans Inc.